
Recently Redhill announced results in July 2018 for a Phase III trial for their drug RHB-104. RHB-104 is an oral pill (no infusions or shots) that uses a combination of antibiotics to treat Crohn's disease. The thinking behind the drug is that Crohn's is a bacterial infection caused by mycobacterium avium subspecies paraturberculosis (known as MAP for short) which is an infection often found in animals. This infection is believed to contribute or cause Crohn's disease. The theory if you have a medication of anti-MAP it can get rid of the infection and put the Crohn's into remission.
I documented in this post of a woman named Julie Doyle who had surgeries and had tried Humira, Remicade, and every other therapy for Crohn's and then finally tried the anti-MAP therapy (similar RHB-104) and within 6 weeks Julie added 10 pounds and within one year she had a colonoscopy that showed the Crohn's was in remission. This presentation shows patients that have taken RHB-104 with the before and after photos of the colonoscopy. This article discusses a man in Australia who took 45 minutes to get out of bed from his Crohn's and unable to function until he took an anti-MAP therapy and has been off medications for over a decade and has an "unrestricted life". This presentation discusses a man named David who has been in remission for anti-MAP therapy since 1996. Although, these are only anecdotal stories it is important to know that this therapy has literally changed the lives of individuals and families.
The results of the most recent RHB 104 study showed that after 26 weeks the percentage of patients that had remission was 37% vs 23% for the placebo group. The percentage of people achieving remission from weeks 16 to week 52 taking the medication was 18% vs a 9% for the placebo. If someone who had been flaring for years had almost a 1/5 chance of finally being in remission I would ask my doctor how to get that medication. At the 1 year mark 27% of individuals were in remission vs 20% (this result was not statistically significant)
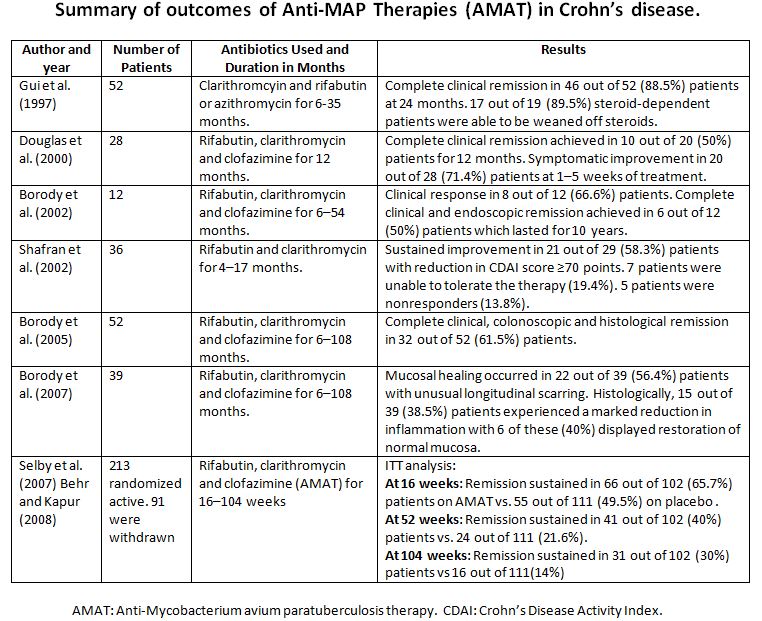
Studies on anti-MAP therapy have been occurring since 1997. Even before this most recent trial occurred over 400 patients had been in clinical trials. The most recent trial for RHB-104 had 331 patients involved which would put the total number of patients over 700. Also it important to note that there hasn't been serious side effects reported with anti-MAP treatment as opposed to the placebo.
Redhill will be meeting with the FDA to discuss a potential approval. I honestly hope the FDA approves this drug as many people suffer from Crohn's: are in misery, have no alternatives, and are open to try this drug. It is important to note that this drug has a pretty good safety profile. The drug has been used in clinical trials and on patients for over 20 years. How much longer do patients suffering have to wait? Another drug to treat Crohn's should always be welcomed as another tool in the tool belt for doctors and patients.
My view as someone who has suffered with Crohn's I have had times when I didn't know when a flare would go away and before I took Humira I can still remember the shooting pain in my stomach that felt like a blunt object stabbing away and having to run to the bathroom urgently. The data shows that RHB-104 and anti-MAP therapy can offer remission to some patients who have tried other medications that have failed. Also given these studies have occurred since 1997 provides years of patient data and to my knowledge there haven't been serious side effects over the years the drug should be approved for patients to see if it can help them. Life is short and we deserve to live the best life possible.









{kind=link}